The Science of Sleep: Optimizing Your Rest for Health and Vitality

How to sleep better is one of the most studied questions in human physiology, and the population-level numbers say most of us are not winning it. According to the CDC's most recent National Health Interview Survey, 30.5 percent of US adults slept less than 7 hours per night in 2024, with 15.4 percent reporting trouble falling asleep most days or every day and 18.1 percent reporting trouble staying asleep (CDC NHIS 2024). Roughly 12.9 percent of US adults used a sleep aid most days or every day in the previous 30 days — 5.2 percent prescription, 5.7 percent over-the-counter or supplements, and 3.7 percent marijuana or CBD (CDC NCHS Brief 116). These are large numbers, and they are not improving.
This is the part of the wellness conversation where I think readers most often get bad advice. There is a body of evidence that actually answers the how-to-sleep-better question — sleep stages, light exposure, bedroom temperature, supplement dosing, when to escalate to clinical care. What follows is what the research says, with citations, doses, and times. Where the answer is genuinely uncertain, I will say so. Where the answer requires a clinician, I will say that too.
How sleep is structured: the cycle, the stages, and which habits damage which stage
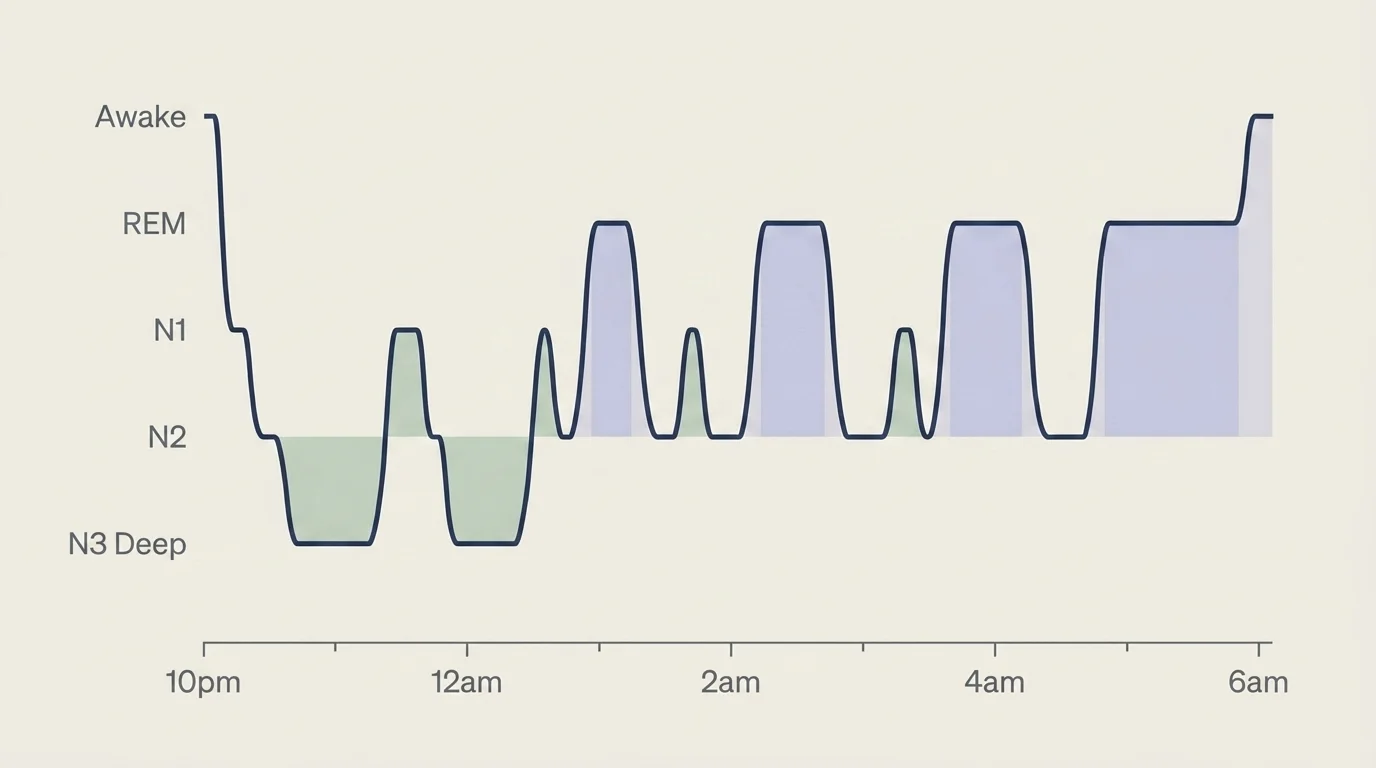
Sleep is not one thing. A typical adult night cycles through four stages roughly every 90 minutes, with four to six complete cycles per night:
- N1 (light onset) — a brief 1-7 minute transition between waking and sleep.
- N2 (light sleep) — accounts for about half of total sleep time; memory consolidation begins here.
- N3 (deep / slow-wave sleep) — the physically restorative stage, dominant in the first third of the night, when growth hormone is released and immune work happens.
- REM (rapid eye movement) sleep — the emotionally and cognitively integrating stage, dominant in the second half of the night, when most dreaming occurs.
The clinically useful version of this knowledge is the habits-to-stages map, which the top-ranking sleep articles consistently fail to make:
- Alcohol within 3 hours of bed → REM suppression. Even one drink reliably reduces REM sleep in the first half of the night, with a compensatory rebound that fragments the second half (Sleep Foundation review).
- Bedroom warmer than about 67°F → less deep sleep. Your core body temperature drops as you fall asleep; a warm room blocks the thermoregulation that lets you stay in N3.
- Caffeine after early afternoon → fewer deep-sleep minutes. Caffeine's half-life is 5-6 hours, so a 3 p.m. coffee still has measurable amounts in your system at 11 p.m. — enough to cut deep-sleep duration even if you fall asleep on time.
- Inconsistent wake time → unstable cycle architecture. Your circadian system organizes around your wake time, not your bedtime; shift the wake time and the entire night's structure shifts with it.
This is the framework underneath every tip below. The interventions that look small individually — cooling the room, cutting caffeine earlier, holding a wake time — work because they each protect a specific stage of the sleep architecture that does specific work.
How to sleep better: 10 evidence-backed practices
A working protocol. Pick two to start; add the rest gradually. The biggest mistake I see is adopting all ten in a week and abandoning all of them by the end of the month.
1. Hold a fixed wake time, including weekends (within 60 minutes). Your wake time is the master signal for your circadian system. Weekend wake-time drift produces social jet lag, which a 2025 meta-analysis in BMC Psychiatry linked to a measurable increase in depressive symptoms in young people (BMC Psychiatry 2025). Aim for your weekend wake time to be within 60 minutes of your weekday wake time.
2. Get morning sunlight within 30-60 minutes of waking. A 2025 study of 1,762 adults found that every additional 30 minutes of morning sun before 10 a.m. shifted sleep onset 23 minutes earlier (BMC Public Health 2025). Aim for 5-10 minutes on a bright day, 15-20 minutes if overcast. Sunglasses defeat the protocol; clear glasses are fine.
3. Cool the bedroom to about 65°F (18.3°C). The consensus range across Sleep Foundation and clinical sleep guidelines is 60-67°F (17-19°C) (Sleep Foundation — Sleep Hygiene). If you cannot drop the room temperature, a fan, a cooling mattress topper, or a hand or foot exposed to cool air outside the covers gets most of the benefit.
4. Cut caffeine at least 8 hours before bed. Caffeine's half-life means a 3 p.m. coffee still has measurable amounts circulating at 11 p.m. This is true even on the nights when you feel sleepy — the subjective sleepiness recovers faster than the deep-sleep impact does.
5. Dim lights and screens 2 hours before bed. Bright evening light suppresses melatonin and pushes the circadian system later. Warm-temperature lamps, dim overheads, and a "night shift" setting on devices help. Reading a physical book in lamp light is the cleanest version.
6. Build a 30-minute wind-down. Low-stimulation activity — reading, light stretching, journaling, a hot shower or bath 1-2 hours before bed (which counterintuitively helps by triggering compensatory cooling). Avoid emotionally activating content. The wind-down is part of the protocol, not optional.
7. Use the 20-minute rule. If you have been in bed awake for more than 20 minutes, get out of bed and do something quiet and low-stimulation until you feel sleepy. Lying awake trying to fall asleep is counterproductive — your brain learns the bed as a place of arousal. This is also Component 1 of CBT-I (more on that below).
8. Get 150 minutes of moderate exercise per week, but not within 2-3 hours of bed. Regular cardiovascular exercise consistently improves sleep depth and continuity in randomized trials. The timing caveat is real for some people; if a late-evening workout is the only time you have, prefer strength or yoga over high-intensity cardio.
9. Limit alcohol within 3 hours of bed, and limit total intake. Alcohol shortens sleep onset (it does help you fall asleep faster) but suppresses REM in the first half of the night and fragments the second half. The cumulative trade is unfavorable for sleep quality, regardless of how much you feel rested in the moment.
10. Consider relaxation techniques for sleep — but only if you actually do them. Progressive muscle relaxation, 4-7-8 breathing (4 in, 7 hold, 8 out, four cycles), or a 10-minute body scan can speed sleep onset. They work best when practiced daily for 2-3 weeks before being relied on as a sleep tool.
Related Article: Microbiome Insights: Revolutionary Findings on Gut Health and Its Impact on Mental Well-Being
Natural sleep remedies and the supplement question
This is the section the top-ranking sleep articles tiptoe around. I am a registered dietitian, so I will be specific about what the evidence actually supports and where the marketing has run ahead of the data.
Magnesium for sleep
A 2025 randomized controlled trial in PMC tested 250 mg of elemental magnesium bisglycinate taken 30-60 minutes before bed for 28 days in 155 adults with self-reported poor sleep. The intervention produced statistically significant reductions in insomnia severity scores compared with placebo (PMC12412596, 2025). That is genuine RCT-tier evidence for a supplement, which is rare in the sleep category.
The label-reading caveat matters: many products marketed as "1,000 mg magnesium glycinate" contain only about 140 mg of elemental magnesium, because the glycinate molecule itself accounts for most of the labeled weight. Read the supplement facts panel for "elemental magnesium" or "magnesium (elemental)" — that is the number that matters. Stay at or below 350 mg of elemental magnesium per day to avoid GI side effects (the National Academies' tolerable upper intake from supplements). Magnesium oxide is poorly absorbed and frequently causes loose stools; bisglycinate is the better-tolerated form for sleep purposes.
Melatonin
Melatonin's evidence is real but narrower than its marketing suggests. The studied dose range is 0.1 to 5 mg, taken 2 hours before desired bedtime, and lower doses (0.3-1 mg) often outperform higher doses for sleep onset because they better mimic endogenous melatonin signaling. The 5 mg or 10 mg supermarket doses are usually a marketing decision, not a clinical one. Melatonin is most useful for circadian-rhythm disorders (jet lag, shift work, delayed sleep phase) and less reliable for general insomnia. Short-term use only; long-term safety data is still thin.
L-theanine, glycine, herbal teas
L-theanine (200 mg, sometimes paired with caffeine for daytime focus) has modest evidence for relaxation but weaker direct sleep evidence. Glycine (3 g before bed) has small studies showing improved subjective sleep quality. Chamomile, valerian, and passionflower teas are pleasant evening rituals — the evidence for them is mostly small open-label studies and supplement-industry trials. They are not dangerous, they are not strongly proven, and the ritual itself probably does as much work as the herb.
Related Article: The Alchemy of Essential Oils: Unveiling the Science Behind Aromatherapy’s Therapeutic Effects
What I would say to a client
If you are paying attention to one supplement, make it magnesium bisglycinate at 250 mg elemental, taken 30-60 minutes before bed, for at least 4 weeks before deciding whether it is working. Read the label for elemental content. None of this substitutes for the behavioral interventions in the section above, and none of it substitutes for a conversation with your clinician if your sleep problems are chronic.
Sleep trackers: what they actually measure
This is the section no top-ranking sleep article covers, and it is the single most asked question in my newsletter inbox.
When consumer wearables are validated against polysomnography — the lab-grade overnight sleep study that is the diagnostic standard — they perform with very different accuracy by device:
| Device | Four-stage classification accuracy vs PSG |
|---|---|
| Oura Ring Gen 3 | ~79.5% |
| Whoop 4.0 | ~69.6% |
| Fitbit Sense 2 | ~61.7% |
| Apple Watch Series 8 | ~50.5% |
Sources: Wearable Sleep-Tracking Accuracy 2024-2025 review.
A few notes that will save you frustration. Apple Watch is best at detecting awake time; Oura and Whoop are best at distinguishing REM from light sleep; none of the consumer trackers reaches the diagnostic accuracy that a polysomnogram does. The right way to use them is for night-to-night trends — is your sleep getting better or worse across two weeks, and what changed? — not as a clinical diagnosis. If your tracker is telling you something concerning about your sleep architecture and the symptoms back it up, that is a signal to talk to a clinician, not to recalibrate by reading the wearable harder.
Two sleep myths worth correcting
A short list of myths that show up most in my reader questions, with the actual evidence.
Myth: "I can catch up on lost sleep over the weekend." Partially, but not as fully as the framing implies. Weekend wake-time drift produces social jet lag — roughly two-thirds of working-age adults in industrialized countries experience some, and more than 80 percent of adolescents experience over an hour of weekly social jet lag (PMC review on social jetlag). The 2025 BMC Psychiatry meta-analysis tied it to elevated depressive symptoms in young populations. Keeping weekend wake time within 60 minutes of weekday wake time produces more durable recovery than sleeping in.
Myth: "5 hours is enough if I feel fine." The CDC short-sleep prevalence numbers (30.5 percent of US adults under 7 hours) are large precisely because people normalize their own sleep restriction. Subjective tolerance to short sleep underestimates objective cognitive and metabolic impact — this is well documented in sleep-restriction laboratory work. If you genuinely thrive on 5 hours, you are a rare outlier — the kind sleep researchers describe as having a genetic "short sleeper" phenotype. If you are most people, you are accommodating, not thriving.
When to get help — and what real treatment looks like
This is the part of the article I want every reader who has been struggling with sleep for more than a few weeks to actually read.
Threshold: if you have had difficulty falling asleep, staying asleep, or waking too early at least 3 nights per week for 3 or more months, this is chronic insomnia — a diagnosable condition that has a recognized first-line treatment.
That treatment is Cognitive Behavioral Therapy for Insomnia (CBT-I), and it is recommended as the first-line intervention for chronic insomnia — ahead of medication — by the American Academy of Sleep Medicine, the American College of Physicians, the European Sleep Research Society, and the World Sleep Society (Sleep Foundation — CBT-I, ACP recommendation). CBT-I has five components:
- Stimulus control — relearning the bed as a place for sleep (the 20-minute rule above is part of this)
- Sleep restriction — temporarily compressing time-in-bed to consolidate sleep, then expanding
- Cognitive therapy — addressing the catastrophic-thinking patterns that develop around sleep loss
- Sleep hygiene — the behavioral environment work covered above
- Relaxation therapy — structured practice of techniques like PMR or 4-7-8 breathing
If you cannot access an in-person CBT-I clinician, digital CBT-I apps like CBT-I Coach (Department of Veterans Affairs, free) and Insomnia Coach received positive efficacy ratings in a 2024 empirical review. Digital CBT-I is meaningfully effective in randomized trials and is the most accessible version of the gold-standard treatment.
Red flag for evaluation: if you snore loudly and have significant daytime sleepiness, ask your primary care clinician about obstructive sleep apnea (OSA) evaluation. OSA is underdiagnosed and contributes meaningfully to cardiovascular and metabolic disease. As a recent development worth noting: in late 2024 the FDA approved tirzepatide (Zepbound) as the first medication specifically for OSA in adults with obesity (Sleep Foundation — GLP-1 for OSA), with documented reductions in CPAP requirement and all-cause mortality in cohort follow-up. This is an adjunct to clinical sleep medicine, not a replacement for it.
What this changes about tonight
Tonight is the right scale for honest sleep advice. If you take one thing from this article: cool the bedroom to around 65°F, hold a fixed wake time tomorrow, and get five to ten minutes of morning sunlight when you get up. That is a small, evidence-backed change you can run for two weeks and assess. Add a second tip after that — caffeine cutoff, or wind-down protocol, or magnesium glycinate at 250 mg before bed — and run that for another two weeks.

If sleep problems persist beyond three or four weeks of consistent behavioral practice, please see a sleep-medicine clinician. CBT-I works. Tirzepatide works for the right OSA presentation. Magnesium glycinate has an RCT behind it. None of this is a moral question, and none of it requires you to suffer through a sleep problem alone for years. Sleep is one of the most modifiable health behaviors there is, and individual sleep decisions — like all chronic-health decisions — belong in conversation with your own clinician.
Frequently Asked Questions
Around 65°F (18.3°C). The Sleep Foundation, Healthline, and clinical sleep guidelines all converge on the 60-67°F range — your core body temperature drops as you fall asleep, and a cool room facilitates that thermoregulation. If you cannot lower the room temperature, a fan, a cooling mattress topper, or letting a hand or foot out of the covers captures most of the benefit.
At least 8 hours. Caffeine's half-life is 5-6 hours, so a 3 p.m. coffee still has measurable amounts circulating at 11 p.m. — enough to cut deep-sleep minutes even when you feel sleepy. This is true even on the nights when you fall asleep on time, because the subjective sleepiness recovers faster than the deep-sleep impact does.
A 2025 randomized controlled trial of 155 adults (PMC12412596) found that 250 mg of elemental magnesium bisglycinate, taken 30-60 minutes before bed for 28 days, produced statistically significant reductions in insomnia severity. Stay at or below 350 mg elemental per day to avoid GI side effects, and read the supplement facts panel — many products labeled '1,000 mg magnesium glycinate' contain only about 140 mg of elemental magnesium because the glycinate molecule itself accounts for most of the labeled weight.
Against lab-grade polysomnography, Oura Ring Gen 3 scores around 79.5% on four-stage sleep classification, Whoop 4.0 around 69.6%, Fitbit Sense 2 around 61.7%, and Apple Watch Series 8 around 50.5%. Apple Watch is best for awake-time detection; Oura and Whoop are best for distinguishing REM from light sleep. Use them for night-to-night trends, not as a clinical diagnosis.
Cognitive Behavioral Therapy for Insomnia is recommended as the first-line treatment for chronic insomnia — ahead of medication — by the American Academy of Sleep Medicine, the American College of Physicians, the European Sleep Research Society, and the World Sleep Society. It combines five components: stimulus control, sleep restriction, cognitive therapy, sleep hygiene, and relaxation therapy. Digital versions like CBT-I Coach (free from the VA) and Insomnia Coach received positive efficacy ratings in a 2024 empirical review.
Partially, but not fully. Weekend wake-time drift produces 'social jet lag,' which a 2025 BMC Psychiatry meta-analysis linked to a measurable increase in depressive symptoms in young people. Roughly two-thirds of working-age adults in industrialized countries experience some social jet lag, and over 80% of adolescents experience more than an hour weekly. Keeping weekend wake time within 60 minutes of your weekday wake time stabilizes the circadian system more than sleeping in.
Each ~90-minute cycle moves through N1 (light onset, 1-7 minutes), N2 (light sleep, about half of total sleep time, where memory consolidation begins), N3 (deep / slow-wave sleep, the physically restorative stage dominant in the first third of the night), and REM (the emotionally and cognitively integrating stage dominant in the second half). You complete 4-6 cycles per night; because REM share grows in the second half, a cut-short morning sleep disproportionately costs REM.
Drop the bedroom to around 65°F, dim lights and screens 2 hours before bed, do 30 minutes of low-stimulation wind-down (reading, stretching, journaling), and use the 20-minute rule: if you have been in bed awake for 20 minutes, get out of bed and do something quiet until you feel sleepy. Lying awake trying to fall asleep is counterproductive — your brain learns the bed as a place of arousal.
5-10 minutes on a bright day, 15-20 minutes if overcast, ideally within the first 30-60 minutes of waking. A 2025 study of 1,762 adults published in BMC Public Health found that every additional 30-minute increment of morning sun before 10 a.m. shifted sleep onset 23 minutes earlier. Sunglasses defeat the protocol; clear glasses are fine.
If you have had difficulty falling asleep, staying asleep, or waking too early at least 3 nights a week for 3 or more months, that is chronic insomnia and warrants a sleep-medicine consultation — CBT-I is the recommended first-line treatment. Also escalate if you snore loudly with significant daytime sleepiness, which is a possible sign of obstructive sleep apnea. As a recent development, in late 2024 the FDA approved tirzepatide (Zepbound) as the first medication specifically for OSA in adults with obesity.
Check Out These Related Articles
The Gut-Brain Connection: Unveiling the Impact of Gut Microbiota on Mental Health

Redefining Nutritional Science: The Role of Epigenetics in Personalized Dietary Recommendations

The Birth of Nutrition Science: From Superstition to Evidence-Based Diets
