Microbiome Insights: Revolutionary Findings on Gut Health and Its Impact on Mental Well-Being

A 2025 meta-analysis of 23 randomized controlled trials in 1,401 clinically diagnosed patients found that targeted probiotics produce a substantial reduction in depression symptoms and a moderate reduction in anxiety symptoms — with one important caveat. The effect was statistically significant only at eight weeks or longer of consistent use. That single finding, from the 2025 Frontiers in Pharmacology review on psychobiotics and depression, is the cleanest entry point to the gut-brain axis and mental health conversation in 2026, because it does two things at once. It establishes that the effect is real in the populations and durations actually studied. And it bounds the effect — modest, dose- and strain-specific, and not equivalent to first-line psychiatric treatment.
This guide takes that calibration seriously. I am a registered dietitian, which means food and gut-microbiome topics sit squarely in my scope; mental-health diagnosis and treatment do not, and I will say so at the appropriate boundary. The interesting questions are how the gut-brain axis actually works (vagus nerve, enteric nervous system, microbial metabolites), what psychobiotics are, which named strains have the strongest human-trial support, what the conditions linked to gut-brain disruption actually are, what to eat, what the 2025 frontiers (fecal microbiota transplantation, GLP-1 medications) are doing to the field, and where the honest limits sit.
How the Gut-Brain Axis Actually Works
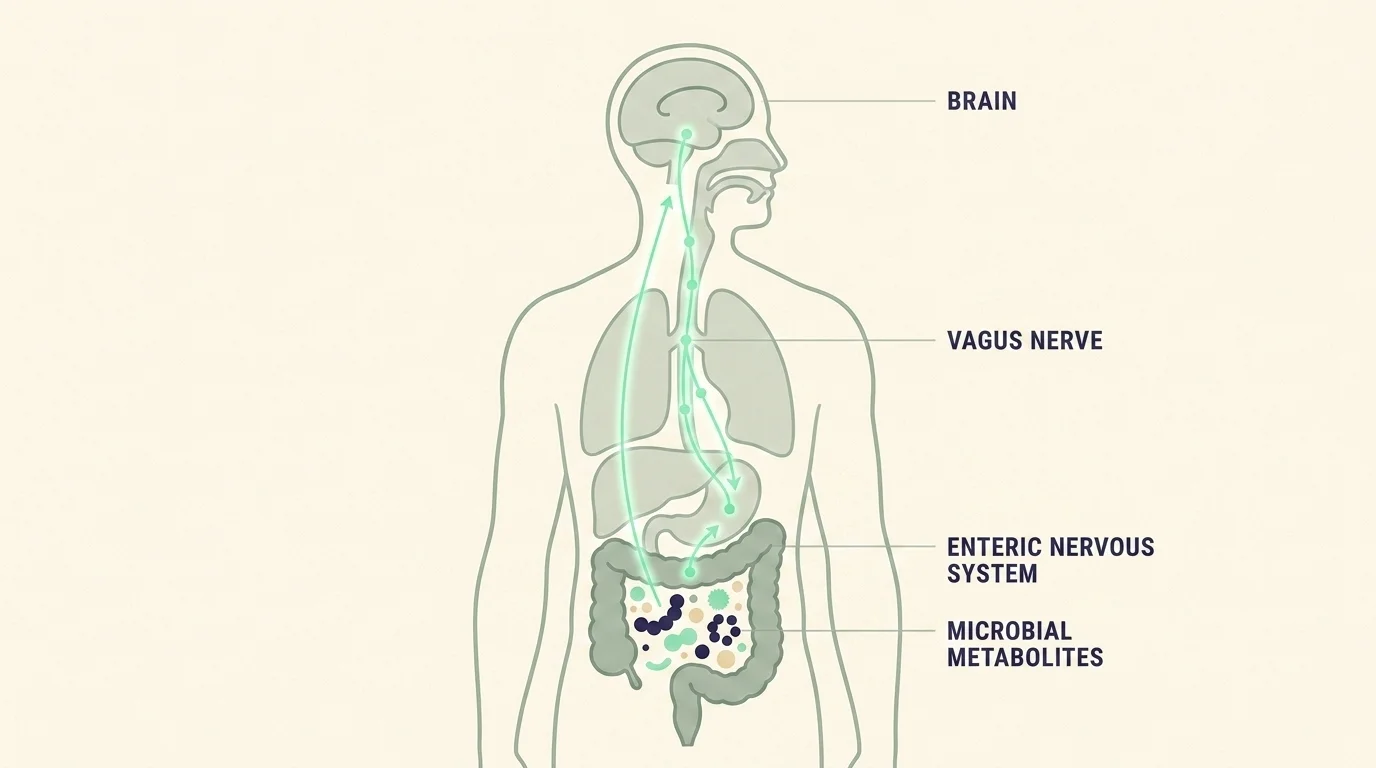
The gut-brain axis is the bidirectional communication system between the gastrointestinal tract and the central nervous system. Three layers do most of the work.
The vagus nerve. The vagus is the primary signaling highway between gut and brain. Per the 2025 PMC review on the vagus nerve in health and disease (PMC12839095) and the 2026 Frontiers in Microbiology psychobiotics review, approximately 80 percent of vagus nerve fibers are afferent — meaning they carry signals from the gut to the brain, not the other way around. That asymmetry is the structural reason microbial metabolites in the gut can directly influence mood, stress response, and cognition. The brain is mostly receiving from the gut, not directing it.
The enteric nervous system. Often called the "second brain," the enteric nervous system is the dense web of approximately 500 million neurons embedded in the lining of the gastrointestinal tract. It can operate semi-autonomously, regulating digestion, motility, and local immune responses without instruction from the central nervous system. The first-brain/second-brain framing oversimplifies the relationship — the two are tightly coupled — but the ENS is real and clinically meaningful.
Microbial metabolites. The trillions of microbes in the gut produce a set of small molecules that interact with the host nervous system. The most important class for mood research is short-chain fatty acids (SCFAs) — butyrate, propionate, acetate — produced when gut bacteria ferment dietary fiber. According to the 2025 PMC paper on circulating SCFAs and depression (PMC12320157), plasma butyrate and propionate are lower in patients with major depressive disorder than in healthy controls, and higher baseline butyrate predicted remission within six months. SCFAs cross the blood-brain barrier, modulate neuroinflammation, and influence the expression of brain-derived neurotrophic factor (BDNF). They are not the only mechanism, but they are the cleanest current biomarker for a microbe-to-mood pathway.
The gut bacteria themselves are not just passive producers of these signals. Many of the same strains can directly produce neurotransmitters. Lactobacillus species produce GABA. Escherichia and Saccharomyces species produce norepinephrine. Bifidobacterium and Streptococcus species produce serotonin. Most of the body's serotonin (often cited as 95 percent) is produced in the gut — though the relationship between gut-produced serotonin and central nervous system serotonin is more complicated than the popular framing implies.
What Psychobiotics Actually Are
The term "psychobiotic" was coined to distinguish probiotics that have demonstrated effects on mental health from probiotics in general. The honest definition: a psychobiotic is a probiotic strain with peer-reviewed human-trial evidence of mood, anxiety, stress, or cognitive effects. Most probiotics on the consumer market are not psychobiotics; some are.
Three named strains (or strain combinations) carry the strongest human-trial support as of 2026.
- Lactobacillus helveticus R0052 + Bifidobacterium longum R0175 — known in the literature as the Messaoudi formula, after the 2011 trial that established its baseline efficacy. A 30-day course in healthy adults produced statistically significant reductions in anxiety, depression, and stress scores. This is the most-replicated psychobiotic combination in the literature.
- Lactobacillus rhamnosus JB-1 — multiple trials showing reductions in anxiety-related behavior and modulation of brain-derived neurotrophic factor (BDNF), with effects mediated through the vagus nerve. The mechanism here is clearest of the three.
- Bifidobacterium longum 1714 — trials showing reduced cortisol response to acute stress in healthy adults and improvements in stress-related measures.
A few honest notes on these. First, "Lactobacillus" alone is not a psychobiotic. The strain matters — different strains of the same species can produce different effects, and a generic "Lactobacillus probiotic" from a grocery store is not the same as L. rhamnosus JB-1 in a clinical trial. Second, the 2025 Frontiers in Pharmacology meta-analysis effect threshold of 8 weeks of use applies to most of the trial evidence. A two-week course is too short to expect significant benefit. Third, the effect sizes across the meta-analyses are modest — meaningful for the populations studied, not a stand-alone treatment for clinical anxiety or depression.
Conditions Linked to the Gut-Brain Axis
The conditions where the gut-brain axis has the strongest research support in 2026:
- Irritable bowel syndrome (IBS). The anchor condition — IBS is increasingly conceptualized as a disorder of gut-brain interaction (DGBI), not a purely intestinal disorder. The vagus-mediated link between psychological stress and IBS flares is well-established.
- Anxiety disorders. The strongest current psychobiotic signal, particularly in generalized anxiety and stress-reactive populations. Effect sizes are modest.
- Major depressive disorder (MDD). The 2025 23-RCT meta-analysis found probiotic supplementation produced substantial symptom reduction in clinically diagnosed depression, with an 8-week minimum effective duration. Important caveat: the comparison is to control or adjunct-to-antidepressant, not to antidepressant monotherapy.
- Autism spectrum disorder. Active research area; gut-brain axis disruption is documented in autism cohorts and several small trials have tested microbiome interventions. The evidence remains preliminary.
- Parkinson's disease. Gut microbiome composition is altered in Parkinson's, and gastrointestinal symptoms often precede motor symptoms by years. The directionality (gut as cause, gut as consequence, or both) is still active research.
- Multiple sclerosis. Documented gut microbiome differences in MS cohorts; therapeutic implications still emerging.
- Functional dyspepsia, chronic fatigue, and other gut-brain interaction disorders. Documented in the 2025 PMC umbrella review on psychobiotics (PMC12845323).
The honest framing on this list: gut-brain axis dysfunction is a real correlate or contributor in all these conditions, and addressing it is a real intervention layer. It is not the whole story for any of them, and treating it as a stand-alone cure is the kind of overreach that gets the broader research category dismissed.
Diet for the Gut-Brain Axis
The dietary patterns with the strongest support for gut-brain axis health break into four mechanism-grouped categories.
Fermented foods (live cultures). Yogurt with live cultures, kefir, kimchi, sauerkraut, miso, kombucha, tempeh. These introduce live microorganisms to the gut. The colonization is usually transient — the bacteria pass through, do some work, and leave — but the metabolic activity during transit produces SCFAs and other beneficial signals.
Prebiotic fiber (feeds beneficial bacteria). Oats, asparagus, garlic, onion, leek, bananas (especially slightly green), chicory root, Jerusalem artichoke, legumes. These are the substrates that feed the bacteria already living in your gut. Prebiotic fiber is, on the current evidence, more important than probiotic supplementation for most people — you cannot meaningfully supplement bacteria into an ecosystem that doesn't have the right food for them.
Polyphenol-rich foods (microbial diversity). Berries, dark chocolate (70% cacao or higher), green tea, extra-virgin olive oil, red wine in moderation, coffee. Polyphenols feed specific microbial populations that increase overall gut microbiome diversity, which is itself a marker of resilience.
Omega-3 sources (anti-inflammatory). Fatty fish (salmon, sardines, mackerel), walnuts, flax seeds, chia seeds. Omega-3s reduce systemic inflammation, including in the gut wall, supporting the integrity of the intestinal barrier.
The pattern across all four categories is more useful than any one food. The most consistent finding in gut-brain axis nutrition research is that dietary diversity matters more than any single intervention — a varied, plant-rich, minimally processed diet outperforms any specific "gut-healthy" food on the metrics that actually correlate with mood outcomes. This is the food-is-not-a-pill framing the literature keeps returning to: the diet pattern is the intervention.
Related Article: The Alchemy of Essential Oils: Unveiling the Science Behind Aromatherapy’s Therapeutic Effects
Emerging Research: FMT and GLP-1 Crossover
Two research frontiers worth knowing about in 2026.
Fecal microbiota transplantation (FMT) for depression. The 2025 PMC meta-analysis of 12 RCTs (n=681) (PMC12536323) found significant reductions in depressive symptoms following FMT compared to control. An active trial — NCT06692361 — is testing capsule-based FMT as adjunct to antidepressants in patients with suboptimal early response. FMT remains experimental for mood indications; it is not yet first-line therapy, and the access pathway outside research settings is narrow. But the data has crossed the threshold from "case reports" to "meta-analysis-level evidence."
GLP-1 medications and the microbiome. The semaglutide/tirzepatide class of weight-loss and diabetes medications alters gut microbiome composition — increasing diversity and shifting toward "leaner-associated" bacterial profiles — per the 2025 Cell Molecular Life Sciences review and the Dr. Kara Fitzgerald January 2026 industry commentary. Some patients report mood improvements on GLP-1 medications independent of weight loss, and microbiome modulation is one of several candidate mechanisms. Human data on this specific mood-via-microbiome pathway is still limited. The FDA has not established causality. The honest framing: the crossover effect is plausible, the mechanism is interesting, the data is preliminary, and any clinical decision about a GLP-1 medication should be made with the prescribing clinician on grounds other than the microbiome story.

Honest Limits and When to See a Clinician
The 2026 evidence base on the gut-brain axis is meaningfully stronger than it was even two years ago. It is also bounded in ways that matter for anyone making real decisions about their mental health.
Effect sizes are modest. The 2025 Frontiers in Pharmacology meta-analysis described psychobiotics as producing "substantial" depression reduction and "moderate" anxiety reduction — but those terms are relative to placebo, not to first-line psychiatric treatment. Psychobiotics in 2026 are adjunctive interventions for mood and anxiety, not replacements for therapy or antidepressants in clinical populations.
Effects are strain-, dose-, and population-specific. A generic probiotic from the supermarket pharmacy is not equivalent to L. rhamnosus JB-1 in a clinical trial. The strain matters, the dose matters, the duration matters (8-week minimum for significant effects), and the baseline population matters (effects are stronger in elevated-stress populations than in healthy low-stress individuals).
Do not stop antidepressants or anti-anxiety medications without medical guidance. If you are currently being treated for clinical depression or anxiety, the right addition of psychobiotics or dietary changes to your routine is a conversation with your prescriber. Discontinuing prescribed psychiatric medication abruptly carries real clinical risks — withdrawal effects, symptom rebound, and in some cases serious safety risks. The supplement layer cannot fix that.
Some populations should consult a clinician before starting probiotics. People who are immunocompromised, critically ill, post-transplant, or pregnant should talk to their physician before starting any probiotic supplement, because the bacteria in even routine consumer products can become a clinical issue when the immune system is not in its usual state.
If you are in crisis, please reach out. Persistent depressive or anxious symptoms that interfere with daily function, sleep, work, or relationships are clinical-grade concerns and warrant a clinician's evaluation, not a probiotic regimen. If you are having thoughts of self-harm or suicide, please contact the 988 Suicide and Crisis Lifeline by call or text. The hotline is staffed 24/7 and connects you to trained crisis counselors. Wellness interventions, including everything in this guide, are not a substitute for crisis care.
The right way to use what is in this guide: as adjunct support, alongside a real care relationship, for people whose mental health is in a workable rather than acute state. If your symptoms are bigger than that, please make the appointment.

A Plainspoken Note on Strains, Doses, and Realism
If you have read this far and you are deciding whether to add a psychobiotic to your routine, here is the version of the recommendation I would give a friend. Eat the food side of this guide first. Add fermented foods, prebiotic fiber, polyphenols, and omega-3 sources to your normal eating over a few weeks. Notice what happens. Most of the gut-brain-axis benefit available to a healthy adult lives in the diet pattern, not in any supplement bottle.
If you decide to try a psychobiotic supplement, pick a product that names the specific strain on the label (not just the genus), commit to at least eight weeks of consistent daily use, and choose a strain with peer-reviewed human-trial evidence for the outcome you care about. The Messaoudi combination (L. helveticus R0052 + B. longum R0175) is the most-replicated choice for general anxiety and stress; L. rhamnosus JB-1 has the cleanest BDNF mechanism story; B. longum 1714 has the cortisol-response data. Read the label, confirm the CFU count, and verify the species — many consumer products advertise generic Lactobacillus without naming the specific strain. A product without a named strain is making a category claim, not a clinical claim.
The honest closer is the same one the literature keeps giving us. The gut-brain axis is real. The diet pattern is the intervention. The supplements have a place at the edge of the diet pattern, with bounded effect sizes, in specific populations, over specific durations. The clinical care relationship is what holds it all together, and the right time to talk to a clinician is sooner than most people do.
Eat the food. Move your body. Sleep enough. Call the therapist. Add the strain if it helps. That is the order that actually matches the evidence.
Frequently Asked Questions
Yes. The vagus nerve is the primary signaling highway between gut and brain, with approximately 80 percent of its fibers carrying messages from the gut to the brain rather than the other way around. That asymmetry is the structural reason microbial metabolites in the gut can directly influence mood, stress response, and cognition. The vagus is the dominant route in the broader gut-brain axis.
All psychobiotics are probiotics, but not all probiotics are psychobiotics. A psychobiotic is a probiotic strain with peer-reviewed human-trial evidence for mood, anxiety, stress, or cognitive effects. The most-replicated example is the Messaoudi formula — Lactobacillus helveticus R0052 plus Bifidobacterium longum R0175 — which reduced anxiety and depression scores in healthy adults over 30 days. Most generic supermarket probiotics are not psychobiotics; some specific named strains are.
Four mechanism-grouped categories: fermented foods (yogurt with live cultures, kefir, kimchi, sauerkraut, miso, kombucha) deliver live microorganisms; prebiotic fiber (oats, asparagus, garlic, onion, leek, banana, chicory root) feeds existing beneficial bacteria; polyphenol-rich foods (berries, dark chocolate 70%+, green tea, extra-virgin olive oil) increase microbial diversity; and omega-3 sources (fatty fish, walnuts, flax, chia) reduce inflammation. Dietary diversity matters more than any single food.
The 2025 Frontiers in Pharmacology meta-analysis of 23 RCTs across 1,401 clinically diagnosed patients found that eight weeks of consistent use is the threshold for statistically significant improvement. Shorter trials often failed to detect the effect. Effect sizes are modest, strain-specific, dose-specific, and stronger in populations with elevated baseline stress than in healthy low-stress individuals.
Diet does not single-handedly cause clinical anxiety or depression, but research consistently links low-fiber, ultra-processed-heavy diets to gut dysbiosis, which is associated with mood disorders via the gut-brain axis. A 2025 PMC paper found that plasma butyrate and propionate — gut-microbe-produced short-chain fatty acids — are lower in patients with major depressive disorder than in healthy controls, and higher baseline butyrate predicted remission within six months. A diverse, fiber-rich, plant-forward diet supports a more resilient microbiome.
For most healthy adults, yes. But people who are immunocompromised, critically ill, post-transplant, or pregnant should consult a clinician before starting any probiotic supplement — the bacteria in routine consumer products can become a clinical issue when the immune system is not in its usual state. Psychobiotics are also adjunctive interventions, not replacements for prescribed antidepressants or anti-anxiety medications. Do not stop psychiatric medication without medical guidance.
FMT transfers gut microbes from a healthy donor to a recipient. A 2025 PMC meta-analysis of 12 randomized trials in 681 participants found significant reductions in depressive symptoms following FMT compared to control. An active US trial (NCT06692361) is testing capsule-based FMT as adjunct to antidepressants in patients with suboptimal early response. FMT remains experimental for mood indications — it is not yet first-line therapy, and access outside research settings is narrow.
Check Out These Related Articles
The Gut-Brain Connection: Unveiling the Impact of Gut Microbiota on Mental Health

Redefining Nutritional Science: The Role of Epigenetics in Personalized Dietary Recommendations

The Birth of Nutrition Science: From Superstition to Evidence-Based Diets
