Cycling for Mental Health: What the Science Actually Shows

Cycling shows up on every "exercise for your head" list, usually with a vague promise that pedaling will fix your mood. The interesting part is that, for once, the research mostly backs the claim — and it's specific enough to act on. Cycling for mental health isn't a slogan: there's population-scale data behind it, named brain chemistry driving it, and a rough dose and timeline you can actually follow. There's also a line where the evidence stops, and an honest guide has to mark that line. So here's what cycling does for your mind, how much it takes, how fast you'll feel it, and where a bike stops being the answer.
How does cycling improve mental health?
Cycling lowers stress hormones and raises the brain chemicals tied to mood: aerobic riding reduces cortisol and increases endorphins, serotonin, dopamine, and BDNF — a growth factor involved in building new neurons (DuVine; UCLA Transportation). That's the mechanism in one breath. The reason cycling specifically tends to stick where other exercise doesn't is mundane and important: it's low-impact, it doubles as transportation, and you can do it at a conversational effort without it feeling like punishment — which means people keep doing it, and consistency is what actually moves mental health.

What the evidence actually shows
Two pieces of recent research do the heavy lifting here, and it's worth labeling what kind of evidence each one is.
The first is population-scale. A 2024 University of Edinburgh study linked census data to NHS prescription records for 378,253 working-age people and found that cycle commuters had about 15% fewer prescriptions for anxiety and depression than non-cyclists over five years, with a larger effect in women (University of Edinburgh / International Journal of Epidemiology). That's a huge natural-experiment cohort — strong for showing a real-world association, though it can't prove cycling alone caused the difference.
The second is a 2026 scoping review in Frontiers in Sports and Active Living that synthesized 87 studies across 19 countries. Psychological well-being improved in 67% of the studies and social well-being in 100%, and the review's summary is quotable: "Cycling is associated with reduced symptoms of depression and anxiety, improved mood, and enhanced emotional regulation" (Frontiers). That's a broad, current synthesis — exactly the citation the typical bike-brand "studies have shown" blog never provides.
The dose, the mechanism, and the timeline
This is the part nobody puts in one place, so here it is as a single protocol. The dosage consensus across current guides is 20–30 minutes of moderate cycling, three times a week, as the entry threshold for a mental-health benefit, with more (45–60 minutes, 3–4×/week) doing more (Canyon).
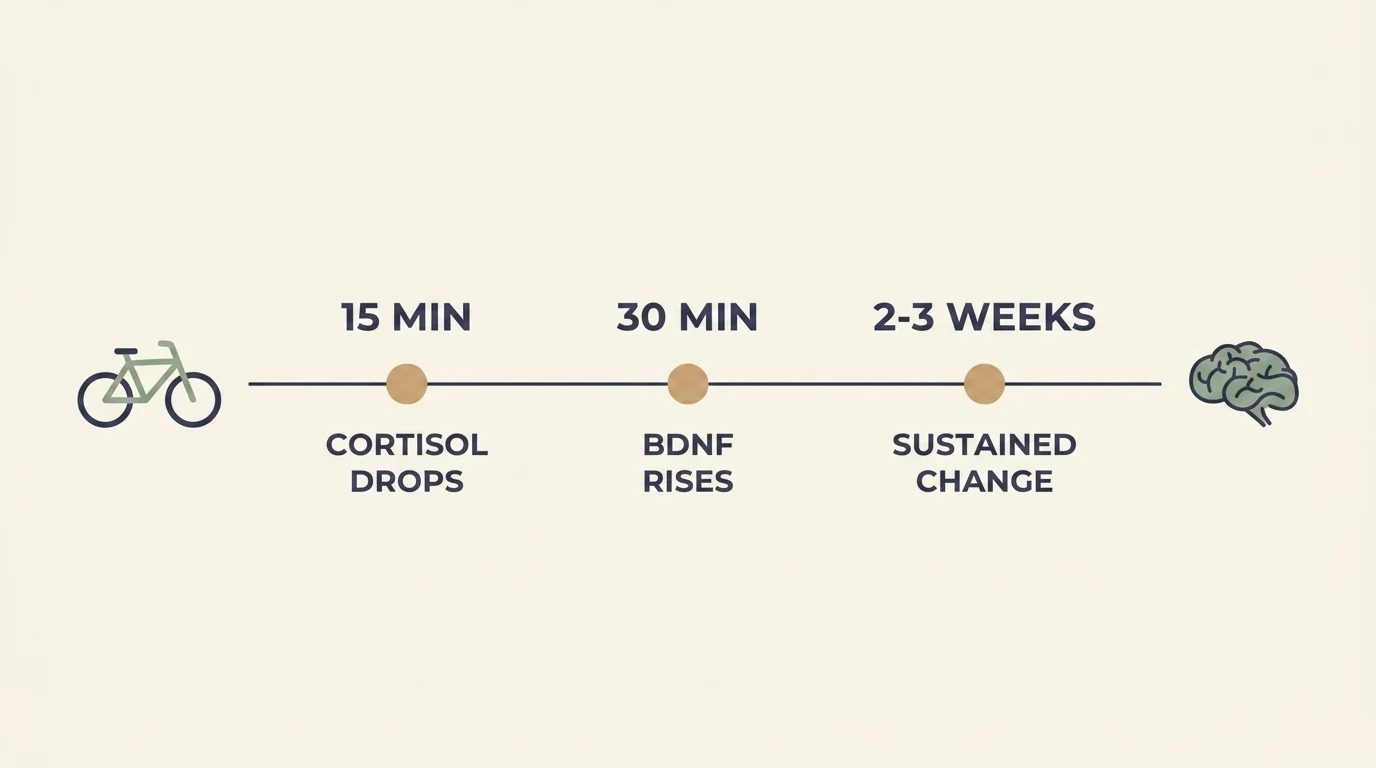
The timeline maps onto the mechanism:
- Within ~15–20 minutes of a single ride: cortisol starts to drop and mood lifts — and that lift from a 20-minute session can last for hours (Canyon).
- After ~30 minutes: one 2020 study found a marked rise in circulating BDNF, the neuron-growth factor (DuVine).
- After 2–3 weeks of regular riding: the sustained, day-to-day mood effects — the ones that show up in the prescription data — begin to settle in (Canyon).
The honest takeaway: one ride buys you an afternoon; three weeks of riding buys you the baseline change. If day 10 doesn't feel transformative, that's the schedule, not a failure.
Cycling for depression
This is where the evidence is most consistent. Across the studies in the Frontiers review that used the Beck Depression Inventory, structured cycling programs of roughly 5 to 16 weeks improved depression symptom scores (Frontiers) — and that lines up with the broader exercise-and-depression literature and the prescription-reduction signal from the Edinburgh cohort. If you're using cycling as part of managing low mood, the practical read is that a sustained program (weeks, not a single ride) is what the depression evidence actually supports. It works best as one reliable, repeatable input alongside whatever care you're already getting — not instead of it.
Cycling for anxiety
Here I have to be straight, because the marketing usually isn't: the anxiety evidence is more mixed than the depression evidence. In the Frontiers review, several cycling studies showed no significant change in anxiety, while one 16-week program did improve it (Frontiers). Plenty of people genuinely feel calmer after a ride — that acute cortisol drop is real — but "a bike ride reliably treats an anxiety disorder" is not something the trials currently support. Treat cycling as a strong, low-risk adjunct for anxiety: useful, worth doing, and not a substitute for evidence-based anxiety treatment.
When cycling isn't enough
No exercise is a magic pill, and saying so is the most useful thing in this article. Even in the positive research, a minority of studies reported negative psychological (~11%) or negative affective (~24%) outcomes (Frontiers) — individual non-response is real, and forcing a ride on a day your body and mind are flattened can backfire. Cycling is also not a treatment for a clinical mental-health condition; it's a powerful adjunct to one.
So, plainly: if you are struggling with persistent depression or anxiety, talk to a doctor or a mental-health professional — cycling belongs in that plan, not in place of it. And if you are in crisis or thinking about harming yourself, in the US you can call or text 988 to reach the Suicide and Crisis Lifeline, 24/7. A bike is a good tool. It is not an emergency service.
How to start
You don't need a coach or a power meter for this — you need a bike that fits and a repeatable slot in your week. Start at the evidence-backed dose: 20–30 minutes, three times a week, at a "could-hold-a-conversation" pace. Ride outside if you can; the Frontiers review found that "positive results were more consistent among outdoor and short- and long-term bicycling interventions" (Frontiers), so the park beats the basement trainer for mood. Build gradually — add minutes before you add intensity — and if a bad knee or a heart condition is in the picture, get cleared by a clinician before you push the pace.
And if a standard bike isn't accessible to you, adaptive cycling counts. As a 2025 review notes, "adaptive cycling holds potential for promoting physical and mental health among individuals with disabilities, who often face barriers to traditional cycling and other forms of exercise" (PMC). The mechanism doesn't care what the bike looks like.

The honest bottom line
Cycling for mental health is one of the better-supported claims in the whole "exercise as medicine" genre: 20–30 minutes three times a week, an afternoon's mood lift from any single ride, real change in two to three weeks, and a 15%-lower prescription rate at population scale. The depression evidence is solid; the anxiety evidence is promising but mixed; and none of it replaces professional care when you need it. Get the bike, ride it at a conversational pace, ride it outside, and give it the few weeks it actually takes — then judge it on what it does, not on what a brochure promised.
Frequently Asked Questions
Yes. Population data link regular cycling to about 15% fewer anxiety and depression prescriptions, working through reduced cortisol and raised endorphins, serotonin, dopamine, and BDNF — though it's an adjunct to care, not a cure.
Mood and cortisol respond within about 15–20 minutes of a single ride, and that lift can last hours. Sustained, day-to-day improvement typically appears after 2–3 weeks of regular riding.
Roughly 20–30 minutes of moderate cycling, three times a week, is the evidence-backed entry threshold, with more (45–60 minutes, 3–4×/week) doing more. Outdoor rides show the most consistent mood gains.
The evidence is more consistent for depression — structured 5–16-week programs improved Beck Depression Inventory scores. Anxiety results are mixed, so treat cycling as a strong adjunct for anxiety rather than a standalone treatment.
No. Cycling is a powerful, low-risk adjunct, not a replacement for professional care. If you're struggling, talk to a doctor or mental-health professional — and if you're in crisis, call or text 988 (US Suicide and Crisis Lifeline).



