Transformative Potential of Psychedelic Therapy: Breakthroughs in Mental Health Treatment Paradigms

A reader emailed me this spring asking whether she should fly her father, who has treatment-resistant depression, to Oregon for a psilocybin session. She had read three viral pieces in a row that described psychedelic therapy as a cure, a revolution, and a paradigm shift. She wanted to know whether any of those words were the right ones, and whether the rest of what she was reading was true.
This is the article I wished I could send her. Psychedelic therapy for depression, PTSD, anxiety, and addiction is one of the genuinely active research frontiers in psychiatry right now, and it is also one of the most aggressively oversold corners of the consumer-wellness internet. Both of those things are true at the same time. I am a dietitian, not a psychiatrist — so my job here is not to narrate clinical experience I do not have. It is to walk you, study by study and approval by approval, through what the evidence currently supports, what it does not, what is legal where you live, and what the safety picture actually looks like in 2026.
If you or someone you love is in crisis right now, please contact the 988 Suicide and Crisis Lifeline in the US (call or text), or your local equivalent. The information below is for orientation, not for self-treatment.

How psychedelic therapy actually works: the three-phase model
Across the major clinical research programs — Johns Hopkins, MAPS, Imperial College London, Compass Pathways — psychedelic-assisted therapy follows a three-phase structure that is genuinely different from how most people imagine it. The drug is not the treatment. The drug is one phase of the treatment.
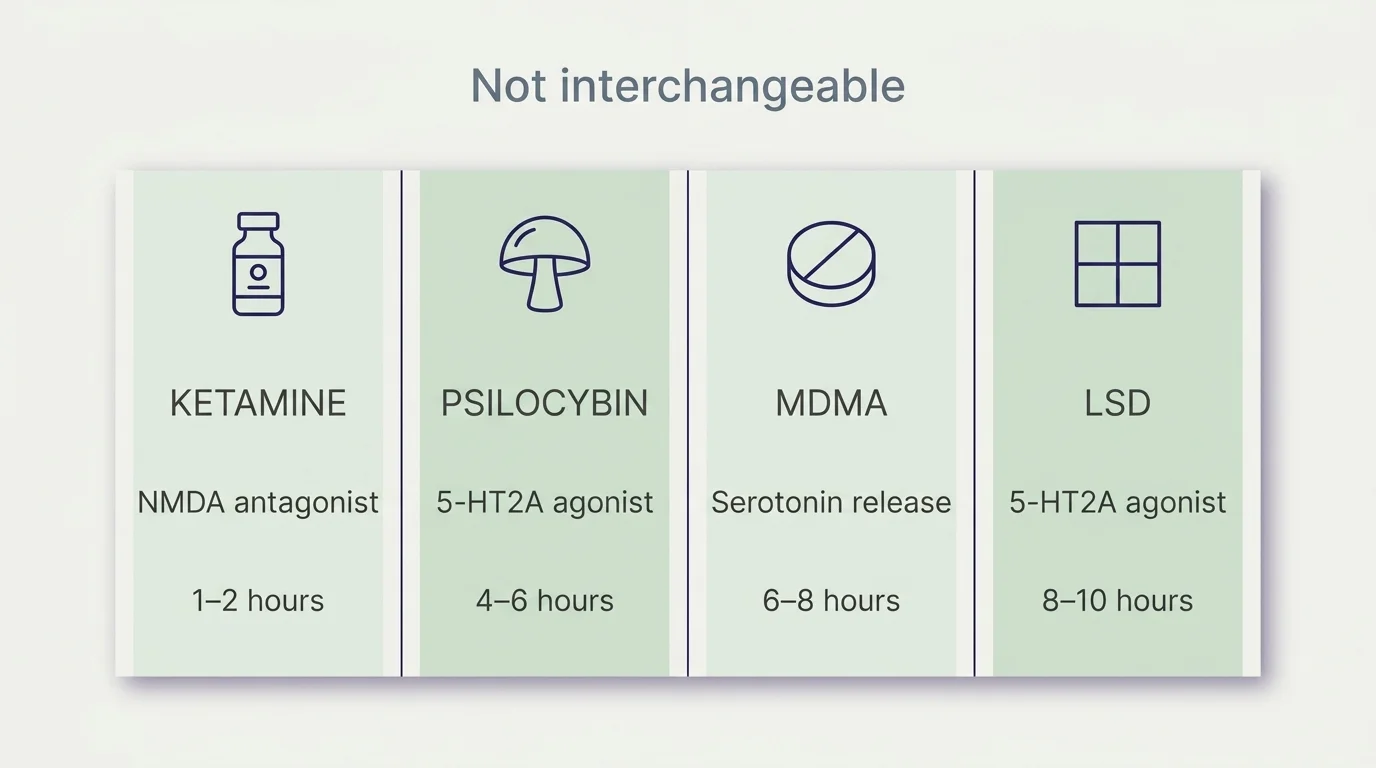
The first phase is preparation: usually two or three sessions with one or two trained therapists over a couple of weeks, building rapport, setting intentions, walking through what the dosing experience will feel like, and screening for contraindications. The second phase is the dosing session itself — a controlled, supervised single experience that lasts somewhere between 1 and 2 hours for ketamine, 4 to 6 hours for psilocybin, or 6 to 8 hours for MDMA, conducted in a quiet, designed clinical space with the therapists present. The third phase is integration: a series of follow-up sessions over the following weeks in which the patient and therapists work through what came up during the dosing session and translate it into behavioural change.
The mechanism the field is converging on is that the dosing experience opens a temporary window of heightened neural plasticity, primarily through agonism at the 5-HT2A serotonin receptor (for psilocybin and LSD) or different mechanisms (NMDA antagonism for ketamine, serotonin release for MDMA), during which existing patterns — depressive rumination, traumatic memory networks, addictive habit loops — become unusually responsive to the integration work that follows. This is part of why every credible program insists the drug only works inside the therapeutic frame, and why home use without preparation and integration is the version of this practice with the worst safety and effectiveness profile.
Substance by substance: a working comparison
The original version of this article mentioned psilocybin and MDMA in a paragraph each and skipped ketamine entirely. Ketamine is the substance the largest number of US searchers are actually asking about, and it is the only psychedelic or psychedelic-adjacent therapy currently legally available across the United States. The honest version of this topic has to cover all four.
Ketamine. Used in psychiatry for treatment-resistant depression, ketamine acts on the glutamate / NMDA system rather than serotonin, and its antidepressant effect can show up within hours. The FDA-approved nasal-spray form, esketamine (Spravato), was cleared in 2019 for treatment-resistant depression under a Risk Evaluation and Mitigation Strategy (REMS) program — it is administered under supervision at certified clinics. Off-label intravenous and intramuscular ketamine therapy is widely available through independent clinics, usually as a series of 6 sessions over 2–3 weeks. Sessions typically run 1–2 hours. Beyond depression, the most striking recent ketamine result is for alcohol use disorder: an Awakn Life Sciences trial reported 86% abstinence at six months post-treatment, compared with 2% pre-baseline and 25% with standard care. That is a striking number from a small program and needs replication; it is also one of the largest signals in addiction medicine in years.
Psilocybin. The active compound in psychedelic mushrooms. Holds FDA Breakthrough Therapy designation for treatment-resistant depression (since 2018/2019). The foundational consumer-facing result is the Johns Hopkins 12-month follow-up of psilocybin-assisted therapy for major depression: 27 participants with chronic depression, 75% response rate and 58% remission at 12 months, mean depression score dropping from 22.8 at baseline to 7.7. Twenty-seven participants is small, the follow-up is durable, and the design was rigorous. Compass Pathways' Phase 3 COMP005 trial — 258 participants across 32 U.S. sites — is reading out in Q1 2026 and is the largest psilocybin trial to date.
MDMA. Empathogen rather than classical psychedelic; mechanism centers on serotonin release. The MAPS-sponsored Phase 3 MAPP2 trial for PTSD enrolled 104 participants and reported 71.2% no longer meeting PTSD diagnostic criteria post-treatment, versus 47.6% in the placebo-with-therapy arm, with complete remission of 46.2% (MDMA) versus 21.4% (placebo). That trial was the basis of the application that the FDA rejected in August 2024 — more on that below.
LSD. Until recently, LSD had little modern controlled-trial data. A 2025 Swiss Phase 2 trial showed two high-dose LSD sessions combined with supportive psychotherapy produced significantly greater and sustained improvements at 3 months in moderate-to-severe major depression, with mostly transient adverse events. This is the first credible modern LSD-for-depression data; it is preliminary, not practice-changing.
Ibogaine, ayahuasca, and DMT are also under active research (ibogaine particularly for opioid use disorder), but the evidence base is earlier and the safety profile of ibogaine in particular includes meaningful cardiovascular risk that puts it outside the consumer-accessible category for now.
Related Article: The Healing Art of Sound Therapy: Harnessing Vibrational Frequencies for Holistic Wellness
Conditions: what the evidence supports
The four conditions with the strongest current evidence are major depression, post-traumatic stress disorder, alcohol and substance use disorder, and end-of-life or cancer-related anxiety.
For psychedelic therapy for depression, the lead evidence is the Hopkins psilocybin follow-up cited above and the Spravato/ketamine approvals already in clinical use. The Compass COMP005 Q1 2026 readout will be the largest single data point this field has produced, and it is worth waiting for before making any major decision.
For psychedelic therapy for PTSD, the MAPP2 numbers above are the lead. The August 2024 FDA decision means MDMA is not currently FDA-approved for general use; the only legitimate access remains clinical trials. PTSD-specific research is also ongoing with psilocybin and ketamine, particularly in veteran populations — the Department of Veterans Affairs committed $1.5M to the first VA-led psychedelic-assisted therapy study, and psychedelic therapy for veterans is a recognized research priority in the April 2026 executive order discussed below.
For addiction and substance use disorder, the Awakn ketamine result for alcohol use disorder is the most striking recent data. Ibogaine for opioid use disorder is an active research area, but the cardiovascular risk profile keeps it outside outpatient settings for now.
For end-of-life and cancer-related anxiety, multiple studies have reported sustained reductions in depression and existential distress in patients with life-threatening cancer following one or two psilocybin sessions, with effects persisting at 6.5-month follow-up.
A note that matters: in every published trial, the comparison group is not "no treatment." It is usually placebo-with-therapy or standard-of-care. The effect sizes above are over and above what current best-practice therapy delivers. They are not over and above doing nothing. Psychedelic therapy is, in every credible framing, an adjunct to and refinement of conventional mental-health care — not a replacement for it.
Current state of approval and access (2026)
This is the section where the field has moved most in the last 18 months, so it is worth being specific.
FDA-approved: Only esketamine (Spravato), the nasal-spray form of ketamine, is FDA-approved for treatment-resistant depression, available through REMS-certified clinics nationwide.
Off-label but legal: IV/IM ketamine therapy at independent clinics nationwide. Not FDA-approved for depression but legal and widely available.
State-regulated programs: Oregon launched regulated adult psilocybin services under Measure 109 in 2023 and is the longest-running such program. Colorado passed Prop 122 in 2022 and is expanding healing-center access through 2025. New Mexico passed the first legislature-driven psilocybin access law in April 2025 (Senate 33-4, House 56-9), targeting December 2026 implementation.
Clinical trials only (US): MDMA-assisted therapy for PTSD; psilocybin for treatment-resistant depression outside Oregon/Colorado/NM programs; LSD; ibogaine; bretisilocin (GM-2505) — AbbVie acquired developer Gilgamesh in August 2025 for $900M upfront ($1.2B total), the first significant Big Pharma move into hallucinogenic compounds.
Recent regulatory milestones: The FDA released its Complete Response Letter on the Lykos MDMA-for-PTSD application in September 2025, citing three concrete issues — failure to systematically collect "positive" adverse events, lack of durability data, and high rates of prior MDMA use among trial participants. Lykos cut roughly 75% of staff and rebranded as Resilient Pharmaceuticals in 2025. In April 2026, an executive order titled "Accelerating Medical Treatments for Serious Mental Illness" directed HHS to allocate $50M through ARPA-H to match state psychedelic research investments and authorized FDA National Priority Vouchers for Breakthrough Therapy drugs, cutting review timelines from 6–12 months to 1–2.
International: Germany established legal psilocybin compassionate access for treatment-resistant depression in July 2025, becoming the first EU country to do so. Australia has allowed psilocybin and MDMA prescribing by authorized psychiatrists since 2023.
The honest summary: ketamine is the only modality you can access through ordinary clinical channels today. Psilocybin services are legal in three states. Everything else is clinical trials, and the largest single data point of the next 12 months is the Compass COMP005 Phase 3 readout.
Related Article: The Power of Hydrotherapy: Transformative Benefits for Physical Rehabilitation & Relaxation
Microdosing: the consumer cousin (and what the rigorous trials say)
Microdosing for depression and anxiety is one of the most-searched adjacent topics and one of the most-misunderstood. The practice — taking sub-perceptual doses of LSD or psilocybin (typically one-tenth of a recreational dose) every few days — has a strong anecdotal following and a weak controlled-trial record.
The most rigorous placebo-controlled microdosing trials have generally shown no significant benefit over placebo on mood, cognition, or anxiety outcomes. The participant-reported effects appear to be largely expectancy effects — meaningful, but not pharmacological. This is the inverse of the clinical PAT pattern, where the therapeutic effect is closely linked to the full psychoactive experience integrated with structured therapy. Microdosing is not a smaller version of psychedelic therapy. It is, on the current evidence, a different practice with different (and substantially weaker) effects.
It also is not legal in most jurisdictions outside the state-regulated programs above, which is worth saying explicitly.
Cost, access, and finding a clinical trial
Cost ranges as of early 2026:
- Ketamine-assisted sessions at independent clinics typically run $400–$800 per session, with a standard course of 6 sessions costing $2,400–$5,000. Insurance coverage is rare for IV/IM ketamine. Esketamine (Spravato) is sometimes covered by insurance.
- Oregon regulated psilocybin services typically run $1,000–$3,500 for a complete preparation-dosing-integration program.
- Clinical trials are free for qualified participants; participants are usually compensated for time and travel.
To find a legitimate clinical trial, the authoritative US source is ClinicalTrials.gov, searchable by condition (depression, PTSD, addiction) and substance. Compass Pathways' COMP005 is running at 32 U.S. sites; MAPS-affiliated MDMA trials are likely to expand following the regulatory shifts above.
If "where can I get psychedelic-assisted therapy" is your real question, the practical answer in most US states today is: a REMS-certified Spravato clinic, a reputable ketamine clinic with a clinical-psychiatry partnership, an Oregon-licensed psilocybin service center if you can travel, or a registered clinical trial. Anything else — a wellness retreat, an underground guide, a friend with mushrooms — is operating outside the safety and integration framework that the published outcomes depend on.
Related Article: Unraveling the Power of Herbal Remedies: Integrating Nature's Healing Wisdom into Daily Life
Safety, contraindications, and the ethics question
This is the section a YMYL-grade explainer cannot skip. Psychedelic therapy is not safe for everyone, and the recent ethics record of the field is more complicated than the marketing suggests.
Cardiovascular contraindications: many of these compounds raise heart rate and blood pressure during the dosing session. Uncontrolled hypertension, recent cardiovascular events, and certain arrhythmias are exclusion criteria in nearly every clinical program.
Psychiatric contraindications: a personal or close family history of schizophrenia, schizoaffective disorder, or bipolar I disorder is a near-universal exclusion from psilocybin and LSD trials, due to the risk of triggering psychotic episodes. Bipolar II is more nuanced and clinically individualized.
Drug interactions: SSRIs and other serotonergic antidepressants interact meaningfully with classical psychedelics and MDMA; MAO inhibitors are an absolute contraindication. These interactions are exactly why the supervised clinical frame matters; this is not a class of drug that pairs safely with a TikTok protocol.
The ethics piece: three MDMA-assisted psychotherapy papers were retracted from Psychopharmacology in 2024–2025 citing "inappropriate physical contact" between trial participants and unlicensed therapists. This was a real and serious credibility hit to the field, and it informed the FDA's caution. It is also why the question of who delivers the therapy — credentialed, supervised, regulated — matters as much as which drug is being studied.
A sober closing
The headline I would write if I had to write one is this: psychedelic therapy is an active, evidence-generating area of psychiatry in which a small number of substances are showing real but not miraculous effects in carefully selected populations under tightly controlled conditions. Ketamine is available now and reasonable to consider with your prescriber if first-line treatments have failed. Psilocybin is on a credible path to FDA approval that may or may not arrive in the next 24 months. MDMA is in a regulatory pause while the field addresses the issues the FDA flagged. Microdosing as a consumer practice is mostly placebo on current evidence. Everything else is research.
Individual mental-health decisions, especially around treatment-resistant depression, PTSD, or substance use, belong in a conversation with a credentialed clinician — preferably one who knows the current state of the evidence and is willing to refer you to a clinical trial if that is the right next step. If you are in crisis, please contact the 988 Suicide and Crisis Lifeline in the US, the Veterans Crisis Line (988, then press 1) if you are a veteran, or your local equivalent. The science is fascinating. It is not yet a substitute for the people who are trained to help you, and it will not become one.
Frequently Asked Questions
Psychedelic-assisted therapies use substances like ketamine, psilocybin, MDMA, or LSD in controlled clinical settings to treat mental-health conditions including depression, PTSD, anxiety, and addiction. The model is not just the drug — it is a three-phase therapeutic framework of preparation sessions, a single supervised dosing session, and integration sessions afterward. The therapeutic effect appears to depend on the full structure, not the drug alone.
The mechanism the field is converging on is that the dosing experience opens a temporary window of heightened neural plasticity — primarily through 5-HT2A serotonin receptor agonism for psilocybin and LSD, NMDA antagonism for ketamine, and serotonin release for MDMA. During that window, existing patterns of depressive rumination, traumatic memory, or addictive behavior become unusually responsive to integration work. Effect sizes are real but not miraculous, and benefits typically depend on the structured therapy that surrounds the session.
Patient safety, therapist credentialing, and access equity are the major concerns. In 2024–2025, three MDMA-assisted psychotherapy papers were retracted from Psychopharmacology citing inappropriate physical contact between trial participants and unlicensed therapists — a credibility hit that informed the FDA's caution. The August 2024 FDA rejection of the Lykos MDMA application cited deficiencies in adverse-event collection and trial design, and the September 2025 Complete Response Letter made those issues public. Credentialed, supervised, regulated delivery matters as much as which drug is studied.
Ketamine-assisted sessions at independent clinics typically run $400–$800 each, with a standard 6-session course costing $2,400–$5,000. Esketamine (Spravato) is sometimes covered by insurance. Oregon's regulated psilocybin services run roughly $1,000–$3,500 for a complete program. Clinical trials are free for qualified participants and usually compensate for time and travel. MDMA-assisted therapy is not yet FDA-approved and is currently only available through clinical trials.
Only esketamine (Spravato), an FDA-approved nasal spray, is legal nationwide for treatment-resistant depression through REMS-certified clinics. Off-label ketamine therapy is widely available through independent clinics. Psilocybin services are legal under state-regulated programs in Oregon (since 2023) and Colorado (since 2025), with New Mexico set to follow in December 2026 after the April 2025 legislation. MDMA-assisted therapy remains in clinical trials following the FDA's August 2024 rejection of the Lykos application.
Ketamine acts on the brain's glutamate / NMDA system and is legally available for off-label use today, with sessions typically lasting 1–2 hours and antidepressant effects that can appear within hours. Psilocybin acts on serotonin 5-HT2A receptors, with sessions running 4–6 hours, and is currently only legal in state-regulated programs (Oregon, Colorado) or via clinical trials. Psilocybin's effects from a single dose can last weeks to months. Both follow the three-phase preparation-dosing-integration model.
ClinicalTrials.gov is the authoritative US source — searchable by condition and substance. Psilocybin currently has more than 39 active trials for treatment-resistant depression and major depressive disorder under FDA Breakthrough Therapy designation. Compass Pathways' Phase 3 COMP005 trial across 32 U.S. sites is among the largest currently running and is expected to read out in Q1 2026.
The evidence is mixed and, on the most rigorous designs, mostly negative. Placebo-controlled microdosing trials have generally shown no significant benefit over placebo on mood, cognition, or anxiety outcomes — the participant-reported effects appear to be largely expectancy effects. Microdosing is also legally distinct from clinical psychedelic-assisted therapy and is not legal in most jurisdictions outside the state-regulated programs.
Check Out These Related Articles

Uncovering Herbal Wisdom: Harnessing the Power of Traditional Remedies for Holistic Well-Being

The Art of Healing: Exploring the Therapeutic Potential of Art Therapy

The Magic of Equine-Assisted Therapy: Harnessing Horse Power for Rehabilitation